Ione Takaki1,
José Scoparo1,
Márcia A Wingeter2,
Cesar Helbel2,
Ricardo A Spironello3,
Roberto KN Cuman3 ![]()
For correspondence:- Roberto Cuman Email: rkncuman1@gmail.com Tel:+554430114867
Received: 17 December 2015 Accepted: 11 April 2016 Published: 27 May 2016
Citation: Takaki I, Scoparo J, Wingeter MA, Helbel C, Spironello RA, Cuman RK. Suppression of HIV-1 viral load after multiple changes in high active antiretroviral therapy: A case report. Trop J Pharm Res 2016; 15(5):1109-1111 doi: 10.4314/tjpr.v15i5.29
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
High active antiretroviral therapy (HAART) can reduce plasma viremia to levels below the limit of detection, leading to adequate immune recovery and clinical stability in most HIV-1-infected patients. However, the virus persists in reservoirs, and free virions can be found in the plasma. We report here the case of an HIV-infected patient diagnosed in 1999, who exhibited good adherence to medication and HAART efficacy after multiple protocol changes. In this study, we describe the clinical features, chronological changes in HIV viral load and CD4+ T-cell count, and treatment outcomes of multiple combinations of antiretrovirals (ARV).The patient presented cycles of viral load during treatment ranging from undetectable, low, and intermediate HIV-1 RNA levels, to levels above the limits of quantification. A therapeutic regimen intensified with raltegravir (RAL) promoted constant depletion of HIV viral load and an increase in CD4+ T-cells. The report shows that enhanced HAART efficacy using RAL can reduce HIV viral load.
Introduction
High active antiretroviral therapy (HAART) has been reported to be efficacious in hastening immunological recovery and symptomatic improvement after antiretroviral therapy (ART). Indeed, an overall good immunological response is observed, with higher CD4+ T-cell counts, temporally and quantitatively. Although ART efficacy controls viremia, many factors and events may necessitate a change in therapy, such as drug toxicity, viral resistance and mutation, treatment adherence, cost, and medical support [1,2].
In spite of significant HIV-related morbidity and mortality, HAART effectively suppresses, but does not eradicate, HIV-1 infection [1]. Low but persistent HIV-1 RNA levels can still be detected in plasma and cellular reservoirs [3,4] even after several years of suppressive HAART, and cessation of treatment invariably results in the resumption of viral replication.
In addition to the persistence of long-lived, latently infected cells, low-level viral replication has been proposed as a mechanism that maintains HIV-1 during HAART. If complete viral replication cycles persist, despite suppressive ART, this would lead to a recurrence of cellular infection and a constant replenishment of the viral reservoir [5,6].
Methods
CASE REPORT
In this case report, we describe the clinical features, chronological changes in HIV viral load and CD4+ T-cell count, and treatment outcomes associated with multiple combinations of ARV in a 46-year-old man. Data collected since 1999, the date of diagnosis, were obtained from medical records in Public Specialities Clinic. The patient received the diagnosis of HIV infection on April 1999 with subsequent medical follow-ups at an average frequency of three times per year for sixteen years. The initial physical examination was normal without any sign of chronic disease, opportunistic infection, or AIDS-defining complications.
The patient began HAART in June 1999 at which time his plasma HIV-1 RNA level was 200,000 copies/mL. The initial ART regimen prescribed included didadosine (DDI) + stavudine (d4T), and a good therapeutic response was observed, including full suppression of HIV plasma viremia and a CD4+ T-cell count >500 cells/µL.
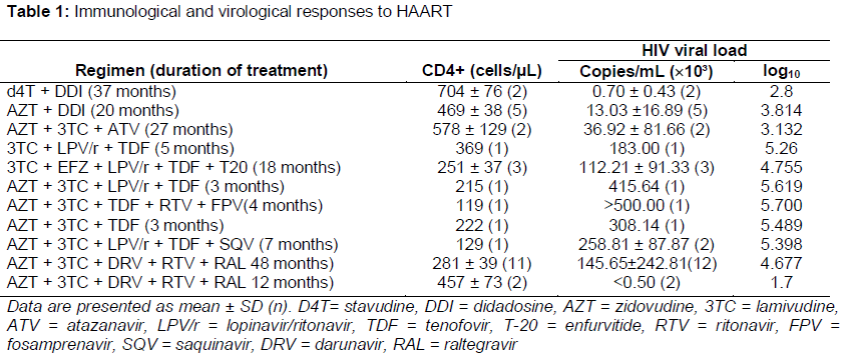
During 16 years of treatment from 1999 to 2015, virological and immunological responses to various combinations of ARV were monitored, and multiple changes were made to the HAART regimen due to increases in HIV viral load, resistance to ARV, and the presence of adverse drug reactions (ADR) ().
In February 2006, when the patient’s plasma HIV RNA level was 183,000 copies/mL, genotypic HIV-resistance test showed resistance-conferring mutations to nucleoside reverse transcriptase inhibitor drugs, but not to non-nucleoside reverse transcriptase inhibitor or protease inhibitor (PI) drugs. Another genotypic HIV-resistance test performed in December 2008 showed no drug resistance mutations to ARV.
During treatment, the patient presented typical signs of ADR: lipodystrophy syndrome, nausea and vomiting, headache, dizziness, tremors, lower limb arthalgia, myalgia, rashes on the limbs, painful nodular erythema, arthritis, and nodules with suppuration of varying degrees of intensity and duration.
Despite these signs of ADR, five years of an HAART drug regimen intensified with raltegravir (RAL) promoted a persistent depletion of the HIV viral load and increase in the CD4+ T-cell count.
Discussion
A major advance in HIV disease treatment occurred with the introduction of HAART, which is sufficiently potent to cause complete and prolonged cessation of viral replication to allow reconstitution of the immune system [5,6]. Despite this progress, only 40 to 50 % of patients in clinical practice are able to achieve maximal and durable suppression of the HIV plasma viral load, and this outcome is a strong predictor of disease control [6].
In contrast to most chronic conditions, successful treatment of HIV infection requires nearly perfect adherence to the treatment regimen to reduce viral load and prevent the emergence of drug-resistant variants, which reduce future treatment options and can be fatal [7-9].
Many studies have suggested that even HAART is not effective for completely eliminating HIV-infected cells, and this could result in viral spreading via privileged anatomic compartments, including various cell populations or tissues[4]. Thus, undetectable viral loads and CD4+ T-cell count values >400 cells/µL, as observed in our patient, indicate the high efficacy of ART. Viral load fluctuation can lead to an increase of HIV viral load, which can occur as “blips,” defined as measurable plasma viral loads (50–1000 copies/mL) that are immediately preceded and followed by viral loads below the detection limit [4,5], which was observed in our patient. The identification and characterization of HIV-1 cellular reservoir(s) in effectively treated patients (HIV-1 RNA below the limits of quantification) is a high priority, and we suggest that this would be an important first step towards the development of a strategy for virus eradication.
RAL belongs to the class of HIV integrase inhibitors, which target a crucial process in the life cycle of HIV. HIV-1 integrase catalyzes the insertion of the viral DNA into the genome of the host cell [9], both in circulating cells and cell reservoirs. Therefore, intensification of the drug regimen with RAL or other drugs could increase the activity of ART and enhance the inhibition of residual viral replication [10].
Conclusion
Administration of the ART regimen, AZT + 3TC + DRV + RTV + RAL, for 5 years suppressed HIV viral load to undetectable levels, suggesting that intensified therapy with RAL promotes persistent reduction of viremia.
References
Archives


News Updates